





anterior uveitis
Management of Anterior Uveitis
Immunomodulatory
therapy is gaining acceptance.
BY
EGIDIO S. FORTUNA, M.D., DAVID HINKLE, M.D., C. STEPHEN
FOSTER, M.D., F.A.C.S
The Standardization of Uveitis Nomenclature (SUN) Working Group devised an anatomical classification for uveitis to serve as a basis for specific uveitis diagnosis. Anterior uveitis is inflammation of the iris or ciliary body including iritis, iridocyclitis and anterior cyclitis.
Epidemiology
The annual incidence of uveitis is between 17 and 52.4 per 100,000 person-years.1-5 It affects those aged 20 to 50. Anterior uveitis accounts for 50% to 92% of all uveitis cases.6 Idiopathic uveitis is the most common form of anterior uveitis in children and adults.
■ Juvenile idiopathic arthritis (JIA). JIA is the predominant systemic disorder associated with uveitis in children. Anterior uveitis is the most common presenting condition, and 80% of cases of anterior uveitis in children are due to JIA.7 The disease is subcategorized as either systemic, polyarticular or oligoarticular in onset.
■ HLA B27 Associated Acute Anterior Uveitis. This is the most common identifiable cause of anterior uveitis, accounting for 18% to 32% of uveitis cases in western countries. It is 1.5 to 2.5 times more common in men than women.8
The typical presentation is that of acute unilateral or bilateral, non-granulomatous anterior uveitis with cellular and protein extravasation into the aqueous humor.6
■ Ankylosing Spondylitis. Acute anterior uveitis may be the first symptom in ankylosing spondylitis, it includes low back pain and morning stiffness with progressive loss of spinal flexibility due to sacroiliitis, lumbosacral spondylitis and progressive spinal fusion. The typical patient is a young male; women frequently have a less fulminant form of disease. Radiographic films of the sacroiliac joint demonstrate sclerosis and obliteration of the joint space. HLA B27 haplotyping is found in 90% of patients with ankylosing spondylitis.
■ Reiter's Syndrome/Reactive Arthritis. This condition presents with the triad of urethritis, arthritis and conjunctivitis or uveitis. It has a male preponderance and occurs between the ages of 15 and 40. It may follow nongonoccocal urethritis in adults or infectious dysentery in children. Nonocular signs include superficial oral ulcers, keratoderma blennorrhagica and circinate balanitis.
|
|
|
Figure 1. Medium-sized keratic precipitates. |

■ Psoriatic Arthritis. Twenty percent of patients with psoriatic arthropathy develop anterior uveitis.
■ Inflammatory Bowel Disease. Five percent of patients with Crohn's disease and ulcerative colitis develop iritis.
■ Fuchs' Heterochromic Iridocyclitis (FHI). FHI is found in 2% of patients with uveitis. Pain and redness are rare. Examination shows small stellate keratic precipitates with fine filaments that are uniformly scattered over the endothelium, with mild anterior chamber inflammation. The affected iris stroma appears atrophic, and the pigment layer often has a moth-eaten appearance at the pupil margin. Posterior synechiae do not develop.
■ Herpes Simplex Virus (HSV). HSV presents as a unilateral recurrent anterior uveitis or iridocyclitis in 85% of cases. Clinical signs include unexplained corneal scarring, decreased corneal sensation, focal or diffuse iris atrophy, iris transillumination defects, anterior chamber cells and granulomatous or non-granulomatous keratic precipitates.
External Exam
Injection of the conjunctiva may be noted, especially perilimbal ciliary flush.
Granulomatous uveitis is characterized by the presence of large, greasy, mutton-fat keratic precipitates. Nongranulomatous keratic precipitates (Figure 1) are small to medium in size.
■ Anterior chamber. The grading schema for intraocular inflammation uses a scale from 0 to 4+. Fibrin exudation occurs when severe inflammation produces significant breakdown of the blood-aqueous barrier and massive protein leakage occurs. Plasmoid aqueous requires aggressive therapy. Hypopyon is frequently seen in Behçet's disease (Figure 2), HLA B27 uveitis and infectious endophthalmitis.
|
|
|
Figure 2. Hypopyon is frequently seen in Behçet's disease. |

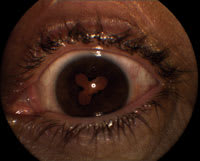
■ Pupil. Inflammation may cause development of posterior synechiae (Figure 3), resulting in irregular pupillary shape and miosis. The iris may also adhere to the trabecular meshwork, forming peripheral anterior synechiae. This can be confirmed by gonioscopic examination and may play a role in secondary glaucoma.
■ Iris. Iris atrophy is best seen using retroillumination lighting. Koeppe's nodules occur on the iris sphincter margin or on the anterior iris surface and are seen in Fuchs' heterochromic iridocyclitis. Bussaca nodules are seen in granulomatous uveitis.
Treatment
■ Mydriatics. Mydriatic agents relieve pupillary sphincter and ciliary muscle spasm, and prevent the formation of posterior synechiae. Cyclopentolate 1% or tropicamide 1% are instilled t.i.d. in acute inflammation or once daily in chronic uveitis.
■ Corticosteroids. Topical and periocular cortico-steroids are the mainstay of treatment. For resistant cases with associated cystoid macular edema, periocular injection with triamcinolone acetonide at 40 mg/mL is delivered through the inferior orbital septum. In severe cases, oral prednisone is given.
■ NSAIDs. Nonsteroidal anti-inflammatory drugs (NSAIDs) reduce the production of eicosanoids through the inhibition of cyclooxygenase (COX). These drugs are an important adjunct to steroids as sparing agents, thereby reducing the total amount of corticosteroid required to eliminate inflammation.
Diclofenac and diflusinal (Dolobid, Merck) are the most effective nonselective NSAIDs, with indomethecin (Indocin, Merck) and naproxen ranking second.
COX-2 selective inhibitors are safer than the non-selective COX inhibitors. Long-term therapy prevents relapse of uveitis in approximately 70% of patients with recurrent non-granulomatous anterior uveitis.
■ Immunomodulatory therapy. Immunomodulatory treatment is indicated when risk factors for vision loss are present or if complete suppression of inflammation cannot be obtained with low-dose corticosteroid therapy.
The risk of adverse effects in chronic corticosteroid treatment in resistant anterior uveitis and the potentially serious side effects of the disease necessitate conversion to steroid-sparing immunomodulatory therapy. Prior to initiation of immunomodulatory therapy, patients must be educated about potential side effects and the necessity for close monitoring. Complete blood counts with white cell differentials, serum creatinine, blood urea nitrogen and liver enzymes are monitored every 6 weeks.
Methotrexate is the drug most commonly used as a corticosteroid-sparing agent because of its low incidence of adverse side effects, once weekly dose and low cost. It is used as monotherapy and in combination with other immunosuppressive agents in induction of durable remission in children and adults.
|
|
|
Figure 3. Inflammation may cause posterior synechiae, resulting in irregular pupillary shape and miosis. |
Methotrexate is a folic acid antagonist that inhibits DNA replication and RNA transcription of dividing immune cells. Hepatotoxicity and interstitial pneumonitis are potentially serious complications, and hence there is a need for close monitoring by an individual who is, by virtue of training and experience, an expert in such matters.
Azathioprine is used as a corticosteroid-sparing agent. It may be combined with low-dose corticosteroid and cyclosporine.9 Azathioprine blocks DNA replication and RNA synthesis, inhibiting proliferation of actively dividing cells. It is used in Vogt-Koyanagi-Harada disease, sympathetic ophthalmia, Behçet's Disease and serpiginous chorioretinopathy.10,11 Potential side effects of azathioprine include nausea, anorexia, hepatotoxicity, myelosuppression with leukopenia and thrombocytopenia.
Mycophenolate mofetil (CellCept, Roche) inhibits inosine monophosphate dehydrogenase, an enzyme in purine synthesis, thereby blocking proliferation of T and B cells.
Mycophenolate mofetil is used in chronic uveitis refractory to azathioprine, cyclophosphamide and coticosteroids. Potential side effects of mycophenolate mofetil include diarrhea, vomiting, leukopenia and increased susceptibility to infection.
■ Signal Transduction Inhibitors. Cyclosporine A is an 11-amino-acid cyclic peptide. It affects lymphocyte proliferation by binding to intracellular immunophilin receptors and blocking Ca-dependent intracellular transcriptional signaling of the nuclear factor of activated T cell (NF-AT).
Potential side effects are nephrotoxicity, systemic hypertension, hirsutism and gingival hyperplasia. Blood pressure and serum creatinine levels must be closely monitored.
■ Cytotoxic/DNA Cross-Linking Agents. Cyclophosphamide plays an important role in severe, sight-threatening forms of uveitis and is reserved for cases refractory to other treatment.10 It is an alkylating agent derived from mustard gas that inhibits T and B cell proliferation. Potential side effects include suppression of testicular and ovarian function, nausea and vomiting, alopecia and bone marrow suppression.
The most serious potential side effects are hemorrhagic cystitis, bladder cancer and other secondary malignancies.12 Due to the potentially serious toxicity, other immunomodulatory agents should be considered prior to cyclophosphamide in treating uveitis.
Chlorambucil (Leukeran, GlaxoSmithKline) is useful in severe cases of ocular inflammation as a second-line agent, particularly in Behçet's disease.9 Chlorambucil is an alkylating agent that cross-links DNA in a fashion similar to cyclophophamide, thereby preventing cell division. The most common side effect is leukopenia.
Potential side effects are increased risk of secondary gastrointestinal and skin cancers, infertility and serious infections. Due to the drug-induced side effects, particularly increased risk of leukemia, long-term, low-dose chlorambucil therapy is not useful in children.13
■ Biological Response Modifiers. New therapeutic options for uveitis are medications targeting specific mediators of the immune response. These molecules block tumor necrosis factor (TNF) alpha (e.g., infliximab) and interleukin-2 receptors (e.g., daclizumab [Zenapax, Roche]).
Infliximab is a chimeric antibody directed against TNF alpha that is administered intravenously every 2 to 4 weeks. Potential side effects include hypersensitivity reactions to the infusion, upper respiratory tract infection and urinary tract infection. There are rare cases of reactivation to tuberculosis, pneumonia, cellulitis and increased susceptibility to infection; however, most studies have demonstrated little toxicity to treatment with infliximab.
Daclizumab is an immunoglobulin G (IgG)
monoclonal antibody. It binds to CD25 of the human IL-2 receptor inT cells,
thus blocking IL-2 intercellular signal to activated
T cells. Daclizumab has
been reported to be effective in the treatment of refractory uveitis and has been
generally welltolerated.14
Prognosis and Complications
Acute episodes of inflammation may be self-limited and benign or may cause complications such as anterior and posterior synechiae leading to secondary glaucoma. Complications of chronic anterior uveitis include band keratopathy, cataract formation, hypotony and phthisis.
Visual loss is more frequent in chronic uveitis. Early recognition, quiescence of inflammation and prevention of complications are critical to preserve good vision, especially in pediatric cases.
Conclusion
Corticosteroids are used as first-line treatment for anterior uveitis. Immunomodulatory therapy represents the standard of care in patients with steroid-dependent and steroid-resistant anterior uveitis. The choice of immunosuppressive agents is complex and depends on the cause and severity of uveitis, the presence or absence of associated systemic inflammation and the patient's response.
Egidio S. Fortuna, M.D., is a research fellow at the Massachusetts Eye Research and Surgery Institute (MERSI). David Hinkle, M.D., is chief fellow at MERSI. C. Stephen Foster, M.D., is founder and president of MERSI.
References
1. Darrell RW, Wagener HP, Kurland LT. Epidemiology of uveitis: incidence and prevalence in a small urban community. Arch Ophthalmol. 1968;68:502-514.
2. Gritz DC, Wong IG. Incidence and prevalence of uveitis in Northern California; the Northern California Epidemiology of Uveitis Study. Ophthalmol. 2004;111:491-500.
3. Paivansalo-Hietanen T, Tuominen J, Vaahtoranta-Lehtonen H,
Saari KM.
Incidence and prevalence of different uveitis entities in Finland.
Acta Ophthalmol Scand. 1997;75:76-81.
4. Tran VT, Auer C, Guex-Crosier Y, Pitet N, Herbert CP. Epidemiological characteristics of uveitis in Switzerland. Int Ophthalmol. 1994;18:293-298.
5. Vadot E, Barth E, Billet P. Epidemiology of uveitis: preliminary results of a prospective study in the Savoy. In: Saari KM, ed. Uveitis Update. Amsterdam: Elsevier Science Publishers; 1984:13-17.
6. Chang JH, Wakefield D. Uveitis: a global perspective. Ocul Immunol Inflamm. 2002;10:263-279.
7. Foster CS. Diagnosis and treatment of juvenile idiopathic arthritis-associate uveitis. Curr Opin Ophthalmol. 2003;14:395-398.
8. Chang JH, McCluskey P,Wakefield D. Acute anterior uveitis and HLA-B27. Surv Ophthalmol. 2005;50:364-388.
9. Okada A. Immunomodulatory therapy for ocular inflammatory disease: a basic manual and review of literature. Ocul Immunol Inflamm. 2005;13:335-351.
10. Jabs DA, Rosenbaum JT, Foster CS, et al. Guidelines for the use of immunosuppressive drugs in patients with ocular inflammatory disorders: recommendations of an expert panel. Am J Ophthalmol. 2000;130:492-513.
11. Djalilian AR, Nussenblatt RB. Immunosupression in uveitis. Ophthalmol Clin North Am. 2002;15:395-404.
12. Talar-Williams C, Hijazi YM, Walther MM, et al. Cyclophosphamide-induced cystitis and bladder cancer in patients with Wegeners granulomatosis. Ann Intern Med. 1996;124:477-484.
13. Kauppi MJ, Savolainen HA, Anttila VJ, Isomaki HA. Increased risk of leukemia in patients with juvenile chronic arthritis treated with chlorambucil. Acta Pediatr. 1996;85:248-250.
14. Papaliodis GN, Chu D, Foster CS. Treatment of ocular inflammatory disorders with daclizumab. Ophthalmol. 2003;110:786-789.